*Click on any yellow text to be linked to the citation*
I covered my concerns for COVID vaccine (gene therapy) effectiveness/safety back on Jan 27, 2021 in this blog post here but as booster shots are now recommended there are some things that you MUST consider. Let me be frank: IF YOU HAVE ONLY BEEN EXPOSED TO THE MAINSTREAM NARRATIVE REGARDING COVID, YOU HAVE BEEN MISINFORMED AT SOME (likely many) LEVELS.
If I were to ask you 2 years ago, do you trust our government and politicians to be truthful and accurately portray situations at hand? What would have been your answer? In my experience most people had a strong conviction that politicians and government officials are not always/ever fully transparent in their message.
But now over the last 2 years the line between government official/politician/policy maker and healthcare provider has been blurred in unprecedented ways. Let that sink in for a moment…
I’m not here to tell you what to do with your health or to point you to perfect research (there isn’t such a thing because of this little variable that can’t be completely accounted for called LIFE) but in order for me to sleep at night, I need you to be aware of some things. Please keep reading. You are NOT wasting your time.
1. These COVID vaccines/gene therapies are NOT as SAFE as the mainstream narrative has led us to believe. At the time of this article there have been 18,853 COVID Vaccine Reported Deaths and 94,537 Total COVID Vaccine Reported Hospitalizations but 2 studies (one by Harvard) show that historically 1% or LESS adverse events are reported to VAERS (even though practitioners are required by law to do so). That being said there has never been a vaccine/gene therapy administered globally in a short time frame like we have seen with these. One can only these reported numbers reflect more than 1% of the actual adverse events.. Click here to see the current stats. Also, see this 5 min video below recapping this interview with Geert Vanden Bossche, PhD, DVM (former head of vaccine research dept at GlaxoSmithKline).
2. These COVID vaccines/gene therapies are NOT as EFFECTIVE as the mainstream narrative has led us to believe. Click here for a short video showing you research on how the vaccine/gene therapies are continuing to come up short/never provided the protection or immunity initially promised/hoped for. *Disclaimer: this is media with very passionate individuals just like mainstream media. Look past the hype and focus on the data being covered. Full episode here. Here’s an analysis of UK data showing the vaccines are NOT saving any lives at all. Here’s an analysis of England data comparing age adjusted all-cause mortality rates in England between vaccinated and unvaccinated.
3. There are MANY other options beyond what the mainstream narrative has covered and the main reason is there is little to no money to be made with these options. Attention goes where money flows! But it doesn’t mean these options are not more safe, effective, or affordable.
As always, you’re NOT ALONE unless you choose to be. COVID is a very conquerable virus, even for those with several comorbidities. We are here to help, pray, and offer as much guidance as permissible. BUT your health is YOUR responsibility. DO NOT, DO NOT, DO NOT reactively rely on your health insurance to take care of you. The consequences may be grave. PLEASE CONTACT US TODAY IF YOU WOULD LIKE TO KNOW MORE ABOUT THE OTHER OPTIONS/PROTOCOLS WE HAVE FOUND TO BE VERY EFFECTIVE.
If you want more: Here is an very concise and well cited article by Dr. Mercola. Abstract here and full article (with citations) below as a PDF. I’ll bold some sections but you really need to read the whole thing. If you’re not familiar with relative risk vs absolute risk watch this short video here.
STORY AT-A-GLANCE
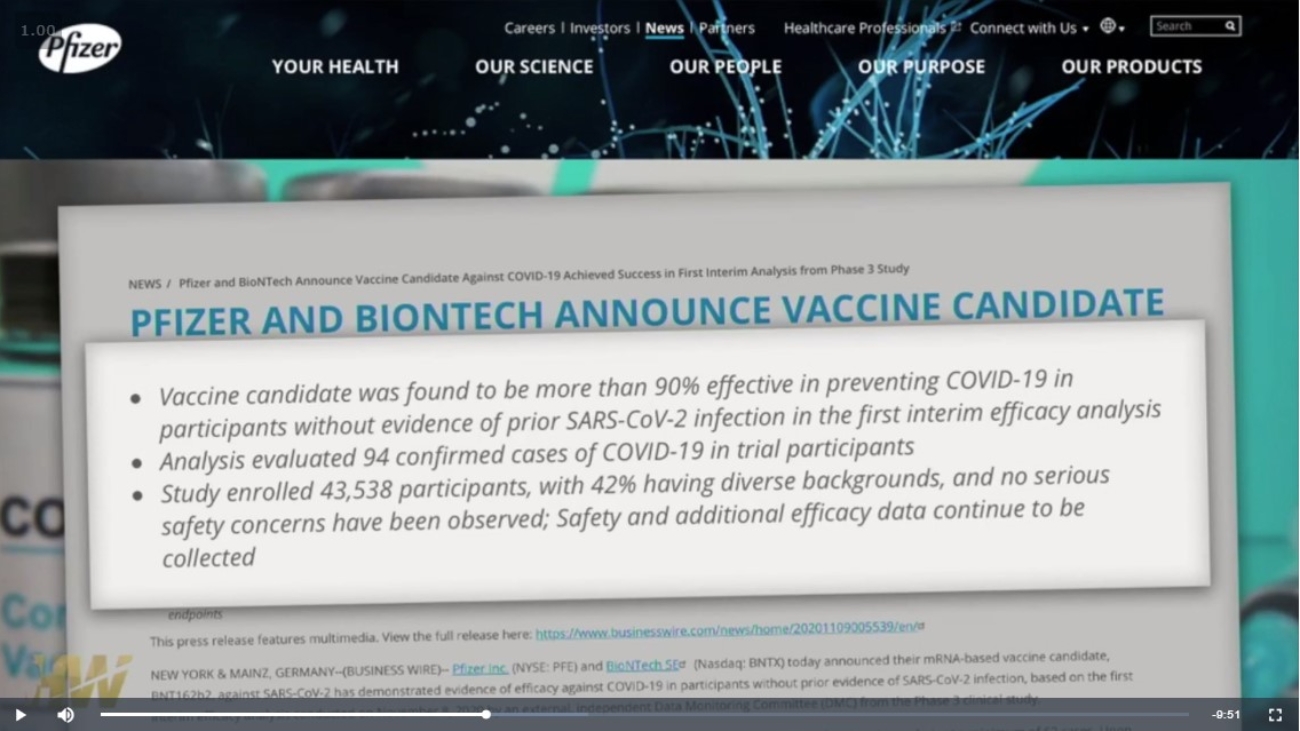
- One of the most commonly used tricks to make a drug look more effective than it is in a real-world setting is to conflate absolute and relative risk reduction. While AstraZeneca boasted a relative reduction of 100%, the absolute reduction was 0.01%. For the Pfizer shot, the relative risk reduction was initially 95%, but the absolute risk reduction was only 0.84%
- In AstraZeneca’s trial, only 0.04% of people in the vaccine group, and 0.88% in the placebo group were infected with SARS-CoV-2. When the background risk of infection is that low, even a 100% absolute risk reduction becomes near-meaningless
- Research shows the majority of SARS-CoV-2-specific antibodies in obese COVID-19 patients are autoimmune and not neutralizing. This means that if you’re obese, you’re at risk of developing autoimmune problems if you get the natural infection. You’re also at higher risk of a serious infection, as the antibodies your body produces are not the neutralizing kind that kill the virus. Does the same hold true for antibodies made in response to the COVID jab?
- At nearly 72%, Vermont has the highest rate of “fully vaccinated” residents in the country, yet COVID cases are suddenly surging to new heights. During the first week of November 2021, cases increased by 42%. The hospital admission rate for fully vaccinated patients increased by 8%, while the admission rate for those who were not fully vaccinated decreased by 15%. Local health authorities blame the surge on the highly infectious delta variant, which would be odd if true, since the first delta case in Vermont was detected back in mid-May
- Data from physician assistant Deborah Conrad show vaccinated people — counting anyone who got one or more shots, regardless of time since the injection — are nine times more likely to be hospitalized than the unvaccinated